

School-based restoration rooms can help ease stress and lessen the impact of trauma for students and teachers.
It is late September at Monroe School, a small elementary school in a low-income urban neighborhood. For the past few years, Monroe has been home to Philadelphia Healthy and Safe Schools (PHASeS), a program that creates trauma-sensitive schools in neighborhoods with high levels of poverty and violence. An initiative of the Temple University Lewis Katz School of Medicine’s Center for Urban Bioethics, PHASeS receives funding from the state of Pennsylvania, the School District of Philadelphia, and other sources. The program assigns trauma specialists to each school, offers professional development, and provides a variety of other services and supports to students, educators, staff, and parents.
Monroe’s leader sought out this program for good reason: Violence is not uncommon in the neighborhood surrounding Monroe, and many students have had traumatic experiences. Indeed, the school had gone on lockdown a week before this September day because of a shooting across the street during school hours. But it is quiet today, buzzing with a low hum of new-school-year energy, as the trauma specialist, Lashay Ward, makes her rounds, checking in with teachers and observing students.
When Ward peeks into a 1st-grade classroom, she notices one student is struggling. Asher’s face is creased in frustration, and he has pushed his paper away. Trouble is brewing at his table. Ward knows Asher has a lot going on at home; he is one of many children, and conflicts between siblings lately have become rough. Ward catches the teacher’s eye, nodding at Asher. When the teacher nods back, Ward gestures to him to follow her out of the classroom.
Asher hunches his shoulders and hangs his head. He says nothing as he walks with slow, heavy steps down the hall and up three flights of stairs. He follows Ward into a formerly empty classroom that has been transformed into a restoration room. It is light and airy. Rugs and brightly colored mats of different textures line the floors. There are art supplies and fidget toys arranged carefully on tables. The room feels well-stocked and orderly.
Asher’s steps quicken as he wanders around the room, picking things up, examining them, putting them down. He seems captivated by the array of objects on the tables. Ward answers his questions in a low, quiet voice but otherwise gives him free reign to explore. As he does, his demeanor begins to change, and he becomes more animated.
A beanbag-toss game in the corner catches his interest. When Ward, seated at a table nearby, says it’s fine for him to take it out, he moves it nearer to her and takes a handful of beanbags. He steps away, tossing the beanbags one at a time into the little holes. At first, he misses each one, but then he gets the hang of it. He smiles with each new success.
As he’s tossing, he says, “I don’t like going to my dad’s house. They’re mean there.” Ward does not react, though she is listening intently. After a moment, she asks, “Why don’t you like going to your dad’s?” He says, continuing to toss the beanbags and not making eye contact, “They fight a lot.” Ward asks gently, “Have you told your mom?” He shrugs and keeps playing. She doesn’t press. Even though he is sharing something difficult, his body, as he throws the bean bags and rushes to retrieve them, seems relaxed.
After a few more minutes, she says it’s time to head back. She helps him put the bean bags away, which he does willingly and efficiently. It has been only 10 minutes since his trudge up the stairs, but he looks different. Smiling and chatting, he follows the trauma specialist back to class.
Understanding trauma
In the language of trauma-informed care, Asher began that exchange in a state of dysregulation. Something had happened at home that left him frustrated and angry. These emotions were so big that he could not manage his thoughts and actions, let alone engage in his schoolwork. Asher needed more than special attention or even someone to talk to. He needed a chance to regulate his mind and body. This is exactly what his time in the restoration room made possible: His physical interactions with the materials in the space and the presence of the trauma specialist, who exuded calm and support, brought him back into a state of regulation. This allowed him to engage productively once more.
Trauma is defined as “not an event in itself but rather the response to a stressful experience” (Cole et al., 2005, p. 18). Studies suggest that as many as two-thirds of children have experienced at least one potentially traumatizing event by age 17 (Perfect et al., 2016). Though trauma can certainly affect children and adults in any family or community, exposure to traumatic experiences and chronic stress is higher in low-income, urban, and minoritized communities, where youth face challenges associated with poverty, structural racism, and violence (Bernard et al., 2021; Bethell et al., 2014; Mathews, Dempsey, & Overstreet, 2009; Stein et al., 2003).
Exposure to traumatic stress can leave a person feeling both powerless and hyper-aroused, with their brain’s stress response so activated that they become agitated and excessively vigilant, seeing danger even where it does not exist (Bloom, 2013). This can make it hard for children to achieve in school (Perfect et al., 2016).
Students who have experienced trauma may behave in age-inappropriate ways in school. They can have short tempers, be distrustful, and have difficulty forming relationships. When they are dysregulated, they may have little tolerance for frustration or be unable to manage challenging emotions. They may also shut down, becoming quiet and unresponsive.
How schools can interrupt trauma responses
If properly equipped with trained personnel and resources, schools can interrupt these patterns and help students learn to regulate themselves and build resilience. In the past 15 years, a number of schools have begun to use their understanding of trauma to design safe, welcoming, and supportive learning communities that encourage students, families, and staff to fully engage in teaching and learning (Cole et al., 2013).
Generally, programs at these schools provide both professional development to educators and trauma-informed programming to students. They may assign to schools trained specialists who can de-escalate conflicts or intervene when someone in the school community becomes dysregulated.
The PHASeS program does all those things. Its professional development sessions help educators understand the signs of dysregulation or other trauma responses, and they provide strategies for helping students and teachers regulate. It also brings trauma specialists like Ward into schools to circulate through classrooms and hallways, checking in with students and adults and intervening to support or de-escalate when possible. PHASeS also creates restoration rooms at each of its schools.
What is a restoration room?
In many schools, restoration or reflection rooms are spaces for discipline. Students who are misbehaving can be sent to this space to minimize disruption in the classroom. But at Monroe and the other PHASeS schools, the restoration room primarily serves as a safe space for de-escalation, regulation, expression, and calm. While emotions, large and small, are welcome and validated, the space helps people learn to manage their feelings and express them in a safe and controlled way. The purpose of the room is not to punish but to help move anyone who is dysregulated back into a mental space that enables them to learn, teach, or interact with others in a productive and healthy way.
Monroe’s restoration room is designed with all these goals in mind. It is orderly, with materials arranged in baskets or bins, and visually interesting, but not over-stimulating. Because trauma so often involves a loss of agency, choice and a sense of control are essential. Thus, there are options for activities, art projects, and games laid out across several tables. There are also choices of places to sit, including soft carpets, bean bag chairs, and stools that sway slightly, allowing someone seated at a table to rock in place (as bilateral and rocking movements can aid in self-regulation).
People who have experienced trauma benefit from a sense of spaciousness, as opposed to feeling crowded or contained. For this reason, furniture is arranged in a way that leaves plenty of room to walk around. Someone who needs to pace or move around could do so easily. Because the body is the physical container of pain, the space must allow for full and free movement. The windows are also often cracked, allowing fresh air in the room, and the door is usually ajar.
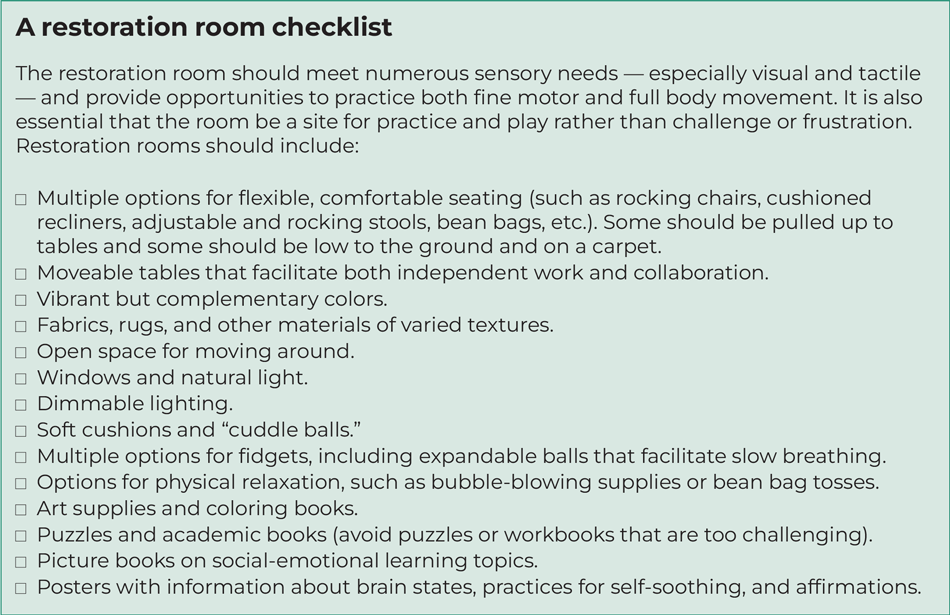
The Restoration Room Checklist can help schools set up their space to support students and staff. The ideal restoration room provides expansiveness, choice, and security. Its atmosphere, especially in contrast with busy and crowded hallways and classrooms, sends a message that people experience viscerally. It speaks to the part of the brain that is assessing whether it is a safe space, clearly communicating that here people can let go of their defenses and take a deep breath.
Of course, the power of the restoration room does not lie in its physical set-up alone. The trauma specialists staffing it are also essential. The staff are trained to withhold judgment and acknowledge that others are experiencing distress without pressing for information, which allows people to feel seen and validated but not vulnerable. Trauma specialists are calm and regulated, and their presence allows others to “co-regulate,” or bring their own bodies and minds back under control.
A space for adults, too
Monroe’s restoration room does not just serve its students. In fact, the PHASeS model is intentional about the need for adults to feel safe and supported. Thus, teachers and school staff also use the room, taking full advantage of its comfortable chairs and art supplies. Some come in when they are feeling anxious or overwhelmed — sometimes seeking to consult with the trauma specialist, sometimes just to breathe and return to a state of regulation.
The trauma specialists also hold professional development sessions for small groups in the restoration room. A visitor to the room during one of those sessions might see a few teachers seated at a table drawing, some stretched out on the rug, and one or two in rocking chairs. Just like the students, adults manipulate the fidgets or test out different mats or chairs, sometimes even removing their shoes or resting with their eyes closed.
Restoration rooms are as important for educators as they are for students. Teachers and other adults in schools may be managing their own trauma reactions that have nothing to do with school. Additionally, the cumulative effects of working with students and families who have experienced significant adversity can affect educators with a form of secondary trauma that undermines physical and mental health. Moreover, life in schools is often stressful, teachers are generally overworked, and the demands on teachers’ time, empathy, resources, and attention are legion. For all these reasons, it’s essential to make sure adults in schools have opportunities to practice self-care and, when faced with challenging situations, to return themselves to a state of regulation.
A safe and healing space
All schools have students who, for a variety of reasons, may have difficulty managing their emotions or may have physical or physiological reactions to traumatic experiences that interfere with their ability to remain engaged in school. Adults too must manage stressful situations, often with limited material and emotional resources.
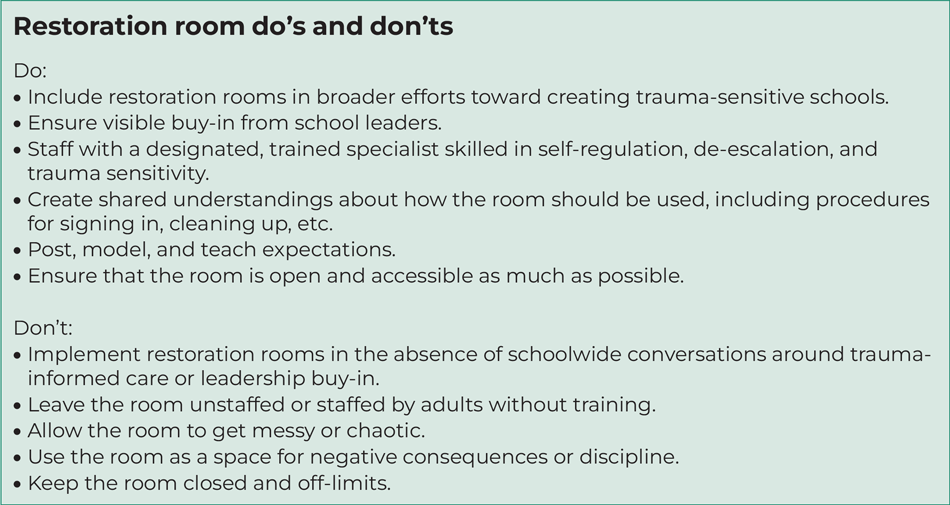
It is not enough for schools to simply offer a space. Restoration rooms must be set up deliberately, with clear guidelines for use, and the school culture must be supportive. Safety, predictability, and consistency are healing for people who have experienced trauma, while uncertainty and disruption can be destabilizing. A well-stocked and thoughtfully designed room that is poorly maintained or chaotic will not serve its intended purpose. Rules and procedures around restoration rooms should be developed to create orderly, safe spaces where visitors know what to expect and how they should engage. The Restoration Room Do’s and Don’ts list on p. 47 can provide guidance.
The promise of trauma-informed schools lies in their potential to become places of safety and healing for everyone. Adding a restoration room does not make a school trauma-informed. But, within a broader effort aimed at helping schools be more responsive to trauma — in students and adults — a restoration room can play an important role.
References
Bernard, D.L., Calhoun, C.D., Banks, D.E., Halliday, C.A., Hughes-Halbert, C., & Danielson, C.K. (2021). Making the “C-ACE” for a culturally-informed adverse childhood experiences framework to understand the pervasive mental health impact of racism on Black youth. Journal of Child & Adolescent Trauma, 14 (2), 233-247.
Bethell, C.D., Newacheck, P., Hawes, E., & Halfon, N. (2014). Adverse childhood experiences: Assessing the impact on health and school engagement and the mitigating role of resilience. Health Affairs, 33 (12), 2106-2115.
Bloom, S. (2013). Creating sanctuary: Toward the evolution of sane societies. Routledge.
Cole, S.F., O’Brien, J.G., Gadd, M.G., Ristuccia, J., Wallace, D.L., & Gregory, M. (2005). Helping traumatized children learn: Supportive school environments for children traumatized by family violence. Massachusetts Advocates for Children, Trauma and Learning Policy Initiative.
Mathews, T., Dempsey, M., & Overstreet, S. (2009). Effects of exposure to community violence on school functioning: The mediating role of posttraumatic stress symptoms. Behaviour Research and Therapy, 47 (7), 586-591.
Perfect, M.M., Turley, M.R., Carlson, J.S., Yohanna, J., & Saint Gilles, M.P. (2016). School-related outcomes of traumatic event exposure and traumatic stress symptoms in students: A systematic review of research from 1990 to 2015. School Mental Health, 8 (1), 7-43.
Stein, B.D., Jaycox, L.H., Kataoka, S., Rhodes, H.J., & Vestal, K.D. (2003). Prevalence of child and adolescent exposure to community violence. Clinical Child and Family Psychology Review, 6 (4), 247-264.
This article appears in the September 2024 issue of Kappan, Vol. 106, No. 1, p. 44-48.

ABOUT THE AUTHORS

Maia Cucchiara
Maia Cucchiara is an associate professor of urban education at Temple University, Philadelphia, PA.

Mary Beth Hays
Mary Beth Hays is an assistant professor with the Center for Urban Bioethics, at Temple University, Philadelphia, PA.








{kind=link}